Motivation
In the absence of mass testing for the covid-19, the lockdown is an efficient strategy because its expected economic cost is smaller than the expected value of the lives lost in the alternative laissez-faire policy (Thunstrom et al., 2020). Exiting from this stalemate is a complex matter because freeing people from confinement could ignite a second wave of contagion and deaths. Some estimates using Markov pandemic dynamics suggests that in the absence of testing and vaccine solutions, strong social distancing measures could last for more than a year (Atkeson (2020), Alvarez et al. (2020)), yielding severe economic and social consequences.
A key element to reduce the economic consequences of covid-19 is the ability to test individuals, given the large prevalence of asymptomatic but highly contagious infected people in the population. Mass reliable testing would allow to free people tested negative to bring them back to work in strategic sectors of the economy, without risking a second wave of contagion. As shown by the experience of South Korea, mass testing is crucial to control the pandemia (Cheong, 2020). As stated by Dewatripont et al. (2020), “restarting production in the economy requires the reliable identification of individuals who will not contract the virus or transmit it to others, whether they have previously displayed the associated symptoms or not”. The extremely limited testing capacity in many countries reduces our expectation of a rapid exit from the current lockdown strategy.
There is thus an obvious argument for a war-like investment plan in the covid-19 testing capacity. This will take some time. In this paper, I propose to complement this medium-term plan with an immediate expansion of the testing capacity by using group testing. It consists in pooling the individual samples that would be tested for the presence of the virus. By nature, the group test is negative if none of the individual samples in the group is infected, and it will positive otherwise. Obviously, this strategy would be particularly useful when the prevalence rate is small. This strategy has been used already in the case of the HIV epidemy (May et al. , 2010). Dorfman (1943) showed that it is a cost-minimizing strategy to detect defects in large populations in various contexts (defects in production, syphilis among army men,…).[1] Contrary to Dorfman, I don’t attempt to identify infected individuals. I rather determine the size of group testing that maximizes the number of individuals whose testing demonstrates they are not infected. This is because the value of information from the test does not come from the treatment of infected people in the absence of an efficient drug to do that. In the context of covid-19, the value of the test rather comes from sending healthy people back to work as soon as possible, without risking infection.
The model and its solution
Suppose that the prevalence rate of the virus in the target population is p. There exists a perfectly reliable test to determine whether the virus is present in a sample, i.e., in a respiratory swab or in a group of such swabs. In the case of group testing, a negative result implies that none of the swabs in the sample contains the virus. A positive result means that at least one swab in the sample contains the virus, but the specific swabs that are infected cannot be identified. The testing capacity is assumed to be extremely limited in the sense that even group testing will not allow for testing the entire population.
I assume that there exists no treatment for the covid. The only benefit of the test is thus to allow people with a negative test to get back to work. I also assume that when a group is detected with the virus, their members remain confined. The scarcity of tests obviously implies that it is better to use a test to detect the virus in another untested group than to try to discover who is infected in a positive group.
In the spirit of Dorfman (1943), I hereafter characterize the size of the group testing that maximizes the expected number of people that can be freed from confinement. Let n denote the size of the groups to be tested. If n is too large, too many groups will be detected with the virus, and that will reduce the expected number of people who will be allowed to get back to work. Technically, the frequency of groups tested negative is equal to (1 – p)n, so that the expected number of people freed from confinement with a single test is equal to N = n(1 – p)n.[2] The optimal size of group testing thus satisfies the following first-order condition:![]() The optimal size of the group is decreasing with the prevalence ratio. It is optimal that the group size be approximately equal to the inverse of the prevalence ratio. The above equation gives us the following expected number N of people back to work with a single test:
The optimal size of the group is decreasing with the prevalence ratio. It is optimal that the group size be approximately equal to the inverse of the prevalence ratio. The above equation gives us the following expected number N of people back to work with a single test: The expected number of people freed from confinement with a single test is decreasing in the prevalence ratio.
The expected number of people freed from confinement with a single test is decreasing in the prevalence ratio.
I can also value the benefit of increasing the testing capacity. To do this, I need to measure the social cost q of individual confinement. Suppose that the optimal confinement strategy in the absence of testing is to remain idle for two months.[3] Therefore, I assume that this social cost equals two months of GDP per capita.[4] For the EU whose GDP/cap is approximately 31.000 EUR per annum, this corresponds to q=5167 EUR. The social value of an individual test is thus equal qN. This should be compared to the cost of producing this test. Table 1 characterizes the optimal strategy for different prevalence ratios.
Table 1: Optimal group testing strategy as a function of the prevalence rate in the target population. I assume that q=5167 EUR.
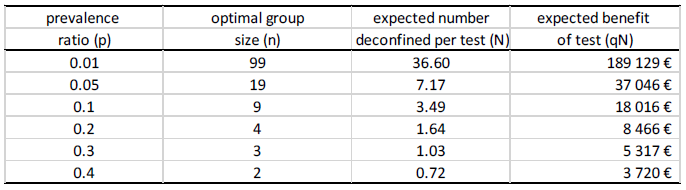
For example, if 5% of the target population is infected, it is optimal to test people in groups of 19. Almost 38% of these groups will be tested negative. In expectation, this will release 7.17 individuals from confinement, thereby generating a social benefit of 37.046 EUR per test. Because the cost of a test is around 40 EUR, expanding the capacity of covid-19 testing is a no-brainer. It is interesting to compare this group testing strategy with the standard individual testing strategy with p=5%. One individual test has 95% chance to be negative. One test can thus free 0.95 individual in expectation. It is thus 87% less efficient than the optimal pooling strategy.
Concluding remarks
Given the extreme economic and social costs of the lockdown, it is crucial to think ahead about an exit strategy. To escape a rebound in the contagion, the only feasible exit scenario is to test people on a massive scale to get people tested negative back to work. Expanding testing capacity by the millions will not be technically possible in the short run. The only alternative is group testing. I therefore propose the following strategy. First, we must solve the problem that nobody really knows the prevalence rate of covid-19 in the population, because tests have most often been targeted to individuals exhibiting symptoms of the coronavirus.[5] So, I propose to test a large representative sample of the population, independently of symptoms.[6] This would allow us to calibrate the prevalence ratio p which is necessary to determine the optimal pooled testing strategy. This will allow us to implement the optimal group testing in a second stage, up to the full testing capacity.
In this paper, I focused on releasing people from confinement, which require testing for the virus. I could have alternatively examined the problem of releasing people who have developed the antibodies, so that they could be used to services to the infected patients without taking the contagion risk. The same logic of group testing could be used for this alternative objective by using serologic group testing to maximize the identification of this group of individuals.
Endnotes
[1] My model differs from Dorfman (1943) by its objective function. Dorfman characterizes a two-stage strategy to identify the infected individuals. It first tests the groups, and then tests all individuals in groups which test positive.
[2] For simplicity, I assume independence of the health status within the group members conditional to belonging to the group.
[3] This is subject to controversy. I rely here on the work by Alvarez et al. (2020) who show using a SIR model (Atkeson (2020)) that a strong confinement rule is optimal for at least two months.
[4] This approach obviously provides a lower bound of the social benefit of exiting from confinement, at least in the early stage of the exit. This is because it will be optimal to target the group testing to people with the most crucial competences for the restart of the economy.
[5] The recent German initiative to randomly test 100.000 people is welcomed.
[6] I am not the only one to recommand this key policy. See for example Dewatripont et al. (2020) and Galeotti and Surico (2020).
Share:



