This is a post about the hard part of the economics of Covid-19. You may think that everything up to now hasn’t been exactly a picnic but from a hard-nosed perspective, big challenges await. There are two: (1) we need to minimise the short-term (this year’s) cost of the pandemic and (2) we need to minimise the medium-term (after this year’s) cost of the pandemic. Not surprisingly, the two are in conflict with one another. In this post, I will explain that the mentality of everyone is to move to a war footing — especially from governments. We have seen a glimpse of this from China in dealing with (1). But we need to worry about (2) as well.
All that said, this post is about the short-term and I will follow up with another about the rest later.
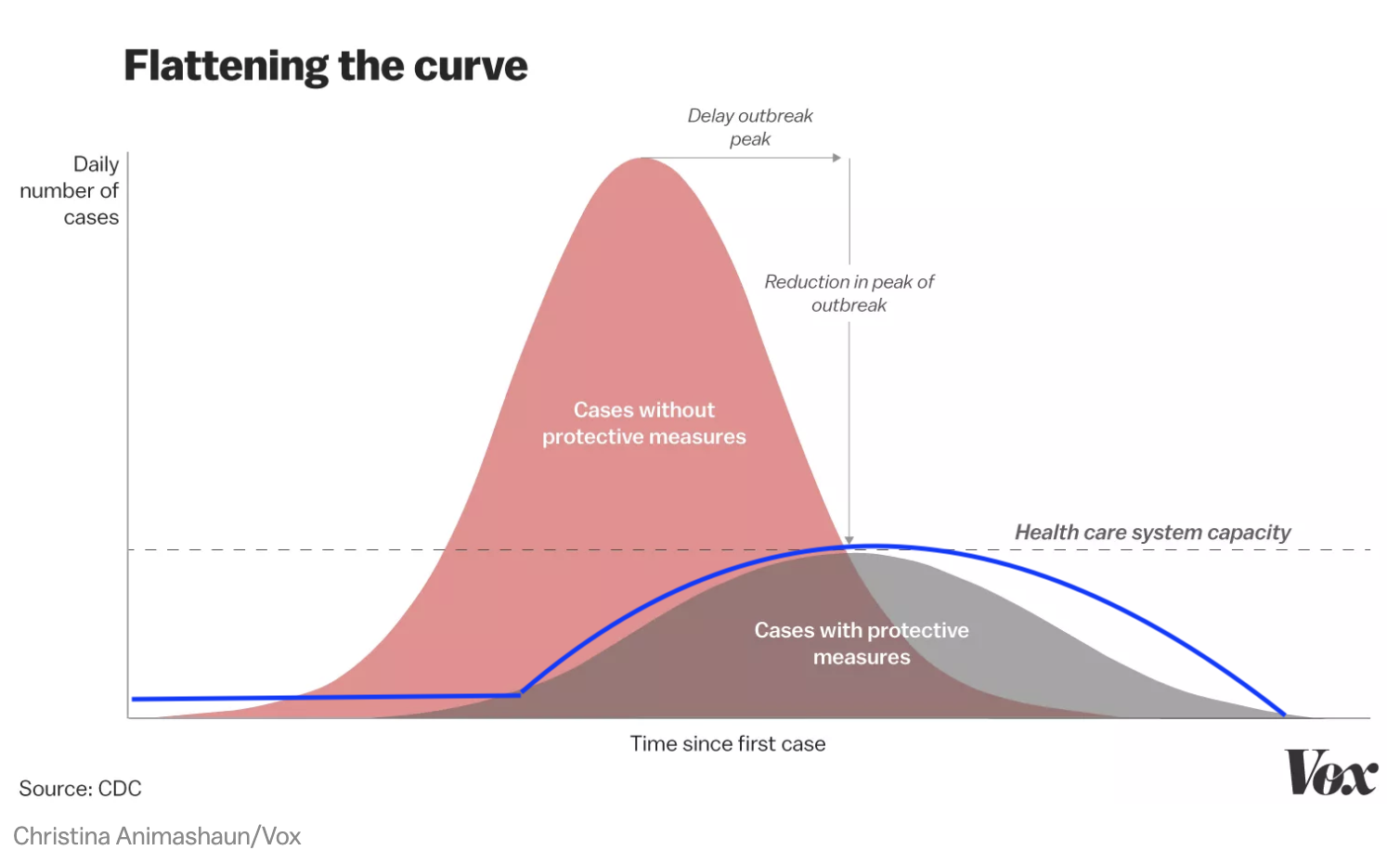
Flattening the Curve is not enough and very costly
By now you have already heard about the main response to the pandemic which is to flatten the curve. That is described nicely in a diagram like this from Vox. The idea is that we reduce the rate of infection through the population which spreads out the time of the pandemic but, most critically, the number of sick at any one time. The rationale for this is that it is very costly to have a high number of sick people at one time. This goes for providing essential economic services but, as this diagram shows, it is really all about health care system capacity. As Italy has shown us, people die essentially because they cannot get hospital-level care. If the infection rate is too high, health care capacity becomes quickly overwhelmed and doctors have to engage in triage, a word which now means choosing who will live and who will die.
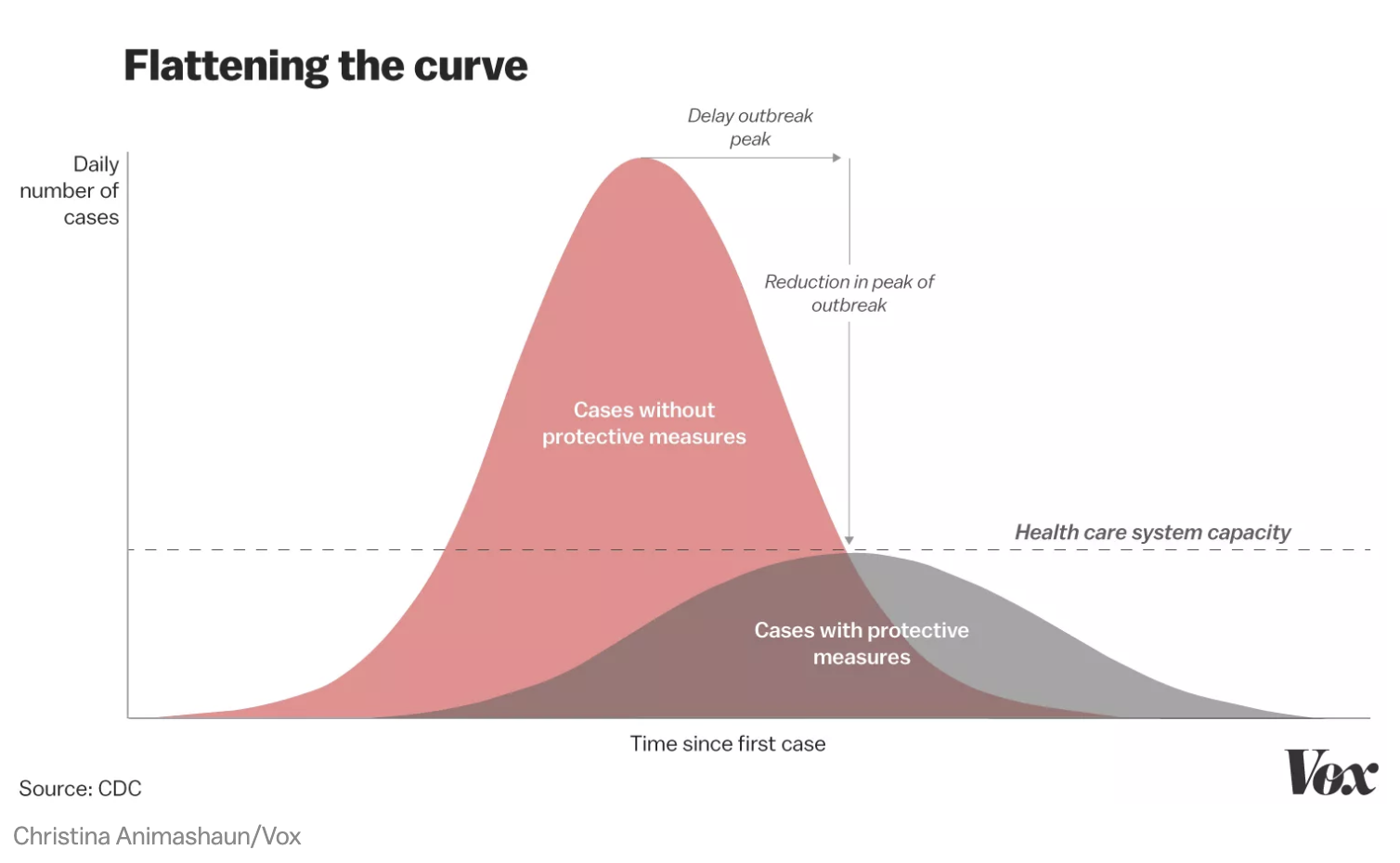
Right now, that message is getting through and the majority of policy focus and activities have been directed at flattening the curve. As my colleague, Kevin Bryan has eloquently described, actions such as hand washing, travel restriction and social distancing, are all aimed at this outcome. We all agree that they needed to begin a week or earlier (regardless of country) but these have been embraced now.
There are, however, costs to this policy which must be traded-off against the benefits. First, flattening the curve extends the short-term disruption — aka how long social distancing must take place and the consequent disruption to life and work. Hence, there will a recession — a downturn in economic activity — not because of some, somewhat mysterious financial force that we usually have but, instead, because we have chosen to reduce economic activity. That is actually good news. For once, this is a recession that economics know how to deal with and agree with one another. (Here is for Bush economic advisor, Greg Mankiw). It isn’t controversial but, as usual, it is challenging to get politicians to adopt the policies.
Second, flattening the curve assumes that you actually don’t go too far and that much of the population actually becomes infected and then immune. Immunity from Covid-19 is still an open scientific question but, let’s assume that is more likely to be true than not. If you reduce the infection rate too far, then most of the population do not become infected and that means that once you stop policies such as social distancing the virus can emerge once more and we all have to do this again. It is a reasonable assumption that we only want to intervene once. Richard Baldwin describes the logic. The concerns are that China, Japan and South Korea may have actually pushed social distancing too far. Israel and now Italy are going even further to keep the virus out altogether.
The reason there is a cost to this is that you are actually more socially useful if you get the virus and are no longer a carrier for the purposes of infection. That means that other people and society do not have to fear interactions with you. In other words, achieving ‘herd immunity’ is an investment in the future. It is like a vaccine but alas you have to actually get the virus rather than an injection. At the moment, as I understand it, the British response to the pandemic is to embrace the idea of ‘taking one for the team.’ That said, a week in bed is one thing. Dying is another. How you conduct this policy without getting significant people in the latter category is hard to see.
Now for the bad news. The flattening the curve diagram is potentially misleading. In fact, it could look more like this:
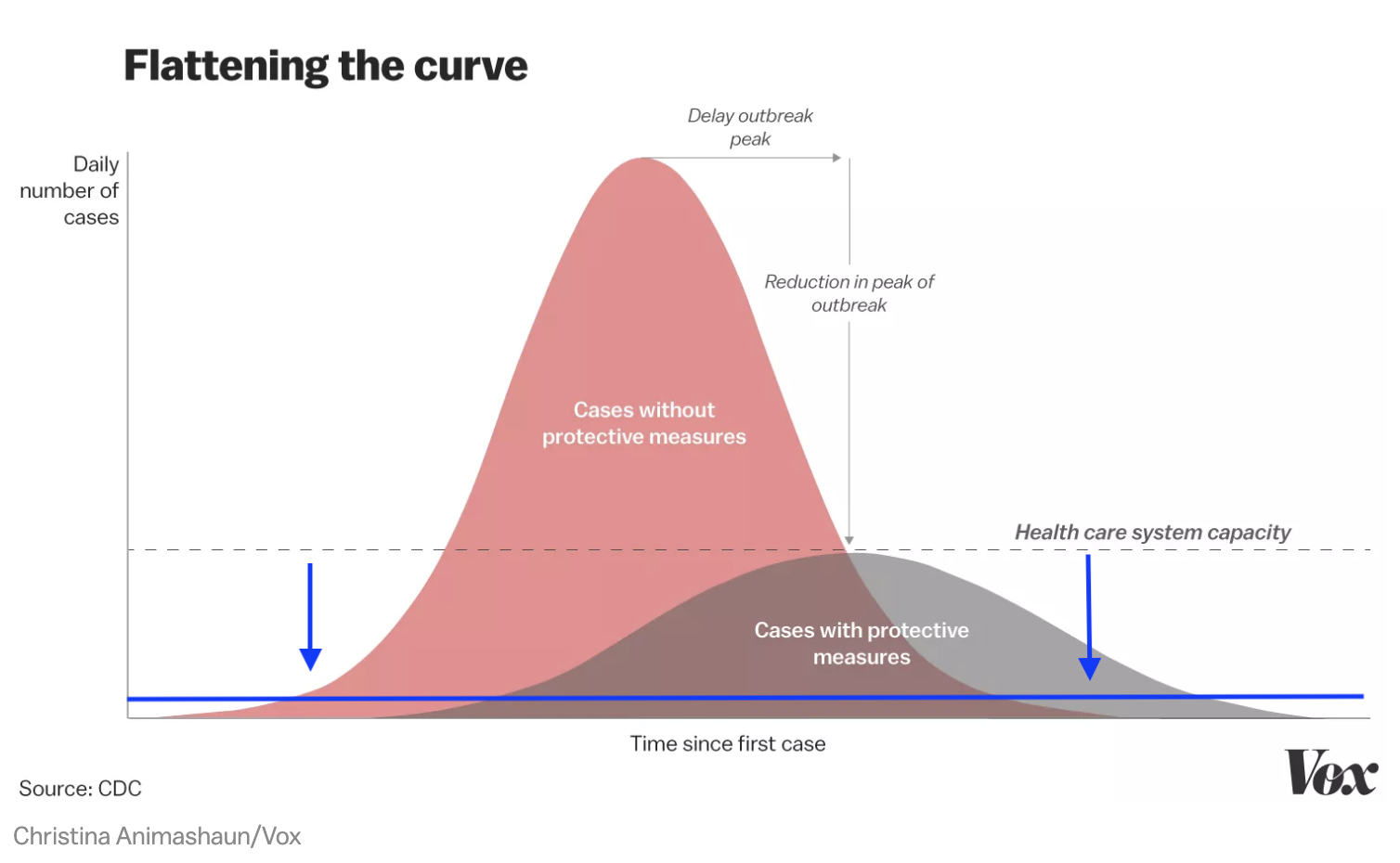
The health care system capacity is likely way lower than the diagram is showing beyond what flattening the curve can actually achieve. This differs by country. But here is the allocation of hospital beds to give you a sense of the problem.
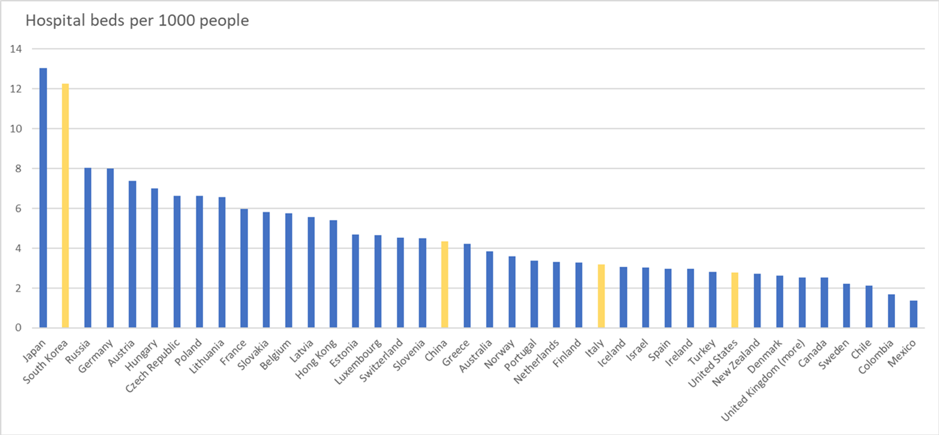
This gives you a sense of the issue. Some countries have four to five times the capacity than others. One imagines that intra-country regional variation is just as big. There are nuances when it comes to ICUs and ventilators, etc. But the bottom line is: even in optimistic flattening the curve scenarios the curve cannot flatten enough. And this constraint is coming up quickly. I did some calculations for Canada and my most optimistic projection had current capacity being overwhelmed in mid to late April. Absent other choices you are left with (a) running out of capacity and having a large share of elderly die or (b) crushing the curve and doing all of this again later in the year. For Europe, North America and Australia, there is no longer a choice and (b) is pretty much off the table.
An Alternative: Dramatic, immediate increase in capacity
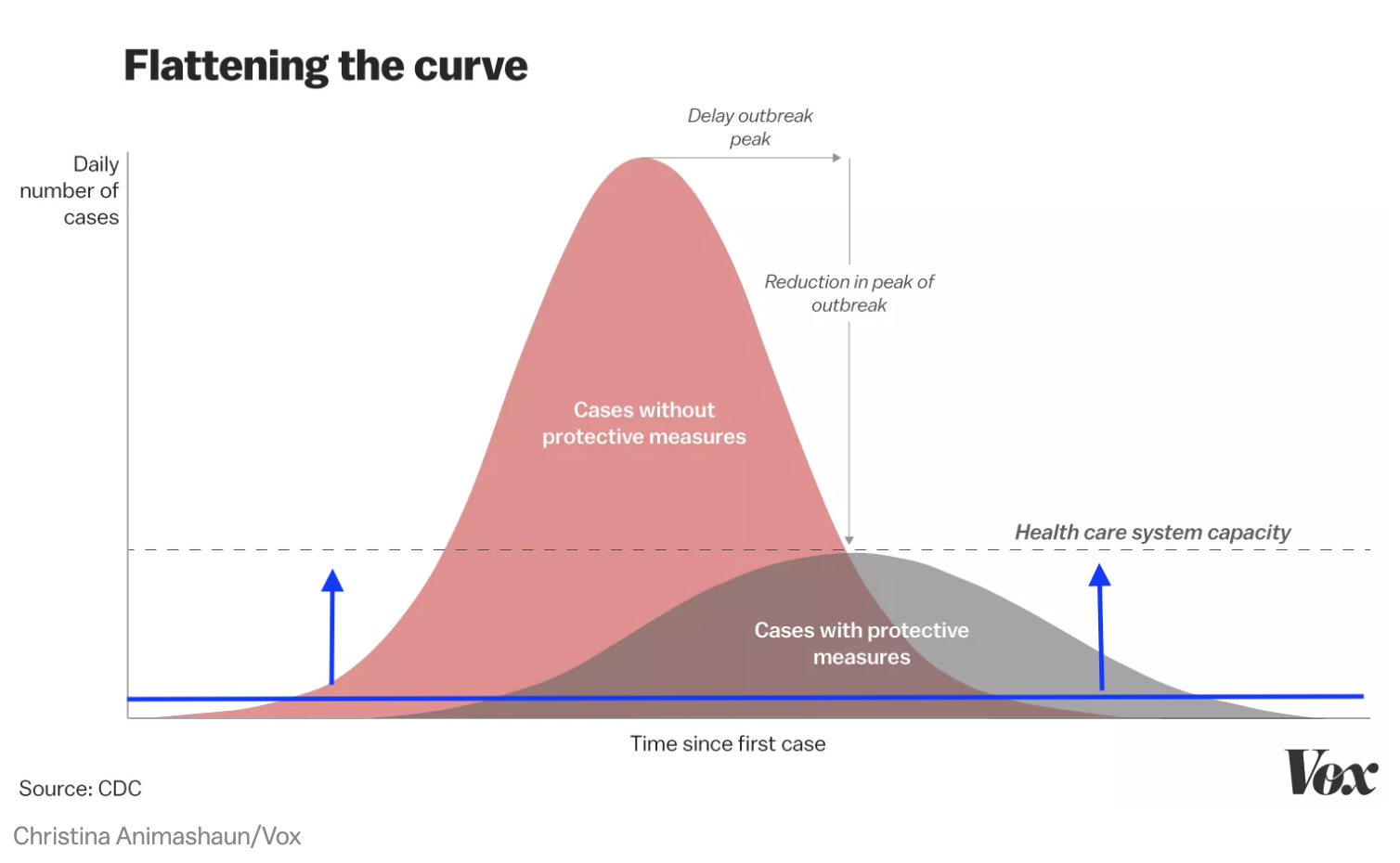
When everything is laid out this way, the policy solution is obvious. If we can’t flatten the curve enough, we must dramatically increase health care capacity. That is,
When China constructed new hospitals in Wuhan in just over a week, this is what they were doing. They did this a month ago and given their stronger infection rate suppression maybe even overdid it. Alas, the projection is that they will likely need that capacity again for round 2. Everyone marvelled at this. I heard: “wow, we can’t do that.” And this was mostly from the health care industry whose basic message for years is how hard it is to provide more. They have had expansion beaten out of them by years of a scarcity mindset.
All that aside: it is very clear that capacity expansion has to be the priority now. It has not seriously been addressed by any government as near as I can tell. Moreover, let’s face it, it will take some time. China impressively did this in a couple of weeks. That will be hard to beat. However, what would Italy have given to have started doing this a couple of weeks ago?
A War Footing
Building out that capacity requires a new mindset and it requires it quickly. The great news is that we — and by we I mean the generation who were adults in World War 2 — have done this before. Entire economies were shifted over to military production. This was done by abandoning market processes of resource allocation and moving to a planned economy. This time around it will be directed towards temporarily and dramatically expanding the capacity of the health care system. The good news is that our military has been doing this too. Perhaps not at this scale but there is critical knowledge and understanding there.
To that end, I believe all governments should consider the following policies:
- Placing the military in charge of health care expansion nation-wide.
- Taking control of all bed, medical device and related manufacturing capacity. I don’t mean this physically but I do mean this in terms of being able to direct activity.
- Putting in place measures to conscript anyone who can be useful in this task. Conscription is an ugly word but you are not sending anyone to fight or die. You are putting people to work. Moreover, we just shut down the Universities and I know we all talk about continuing stuff online, let’s face it, students can do something else for the rest of the year and we will recover. Part of that work could be taking care of dependents while more qualified people do the work.
- This is already happening but there needs to be a Manhattan Project like activity to find a vaccine. The world is going to need it.
That is all just the obvious stuff that comes to my, decidedly non-expert, mind.
In the end, this is what we want to achieve.
The health care system needs to surf the curve (#surfthecurve). This is war and there is no need to keep our plans secret from the enemy.
[Update (14 March 7pm): Not sure of the details yet but Boris Johnson seems to be putting the UK on a war footing along these lines — language and all.]
Share:



